

Motorcycle helmet lying on wet asphalt at night with blurred emergency vehicle lights in background after crash
What to Know About Motorcycle Accident Internal Injuries After a Crash

A rider slides across asphalt after a collision. He stands up, brushes off his jacket, and waves away the ambulance. Three hours later, he collapses in his kitchen from internal bleeding. This scenario plays out more often than most people realize because motorcycle crashes create unique conditions where life-threatening injuries hide beneath intact skin.
The human body wasn't designed to absorb the forces generated when a 400-pound motorcycle traveling at highway speed suddenly stops. Unlike car occupants who have airbags and crumple zones, motorcyclists absorb impact energy directly through their bodies. Internal organs slam against ribcages, pelvic bones, and spinal columns. Blood vessels tear. Tissue ruptures. Yet the rider might walk away feeling nothing more than shaken.
Understanding what happens inside your body during a motorcycle crash could mean the difference between catching a treatable injury and facing a life-threatening emergency hours later when you're alone.
Why Internal Injuries From Motorcycle Crashes Often Go Undetected
The emergency room sees two types of motorcycle accident victims: those brought by ambulance and those who arrive days later, much sicker than they should be. The second group typically made the same mistake—they trusted how they felt immediately after the crash.
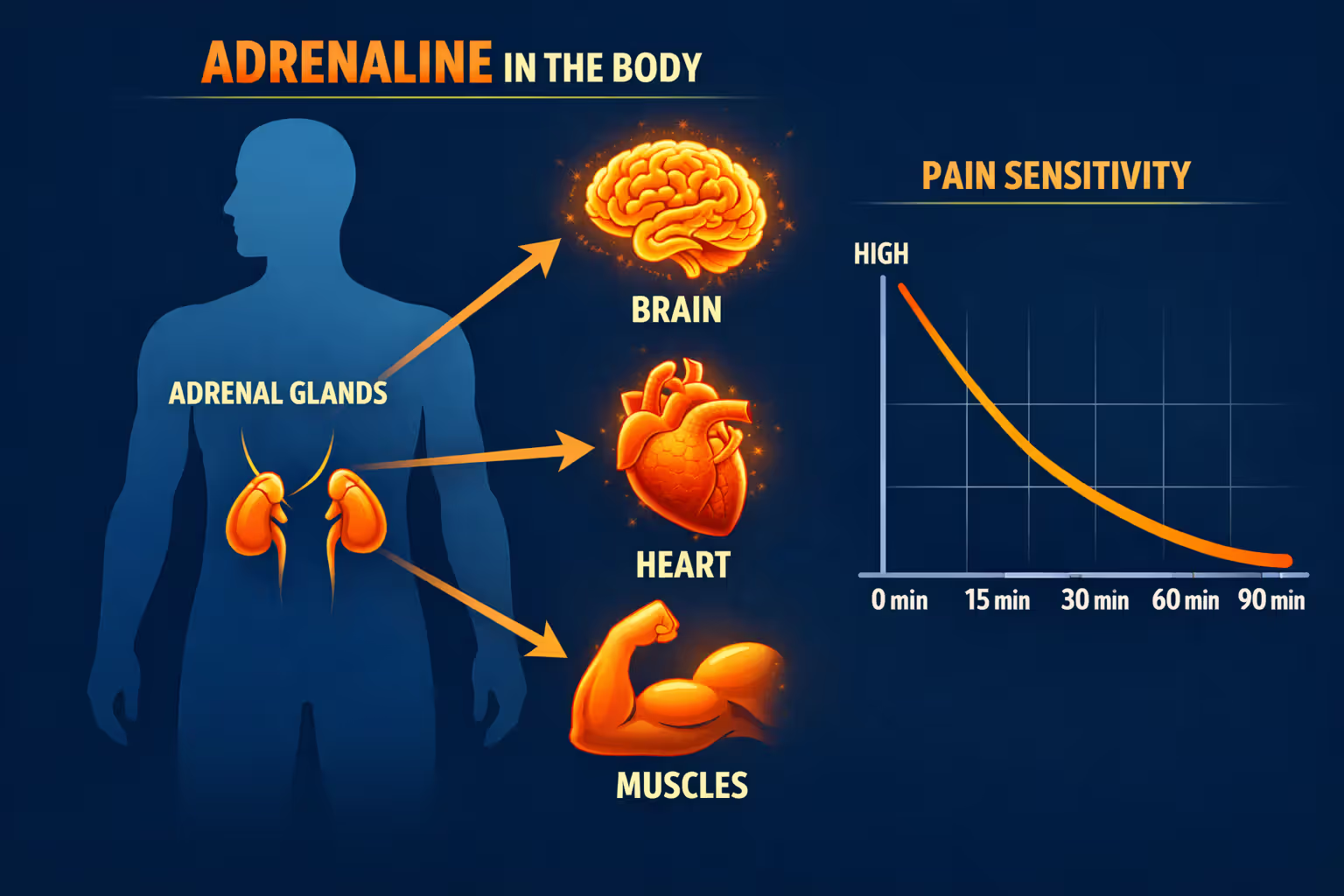
The Adrenaline Masking Effect
Your body floods with adrenaline within seconds of a crash. This stress hormone serves a survival function, temporarily overriding pain signals so you can escape danger. Heart rate spikes. Blood pressure rises. Pain receptors get suppressed. A rider with a ruptured spleen might feel nothing more than mild discomfort while his adrenaline remains elevated.
This biochemical response typically lasts 30 to 90 minutes, sometimes longer depending on the severity of the accident. During this window, a person with serious internal trauma motorcycle accident injuries may walk, talk, and appear completely normal. They decline ambulance transport. They drive themselves home. The adrenaline eventually wears off, and reality sets in—but by then, internal bleeding may have progressed to a dangerous stage.
Emergency medicine protocols assume everyone involved in a significant motorcycle crash has hidden injuries until proven otherwise. That assumption exists because medical professionals have seen too many cases where obvious wellness masked critical damage.
Author: Ryan Whitlock;
Source: spy-delhi.com
Delayed Symptom Onset in Trauma Cases
Some internal injuries announce themselves immediately. Others develop over hours or days through a process called delayed presentation. A small tear in your bowel might leak digestive contents slowly, taking 12 to 24 hours before infection symptoms appear. A liver laceration might ooze rather than gush, allowing blood to accumulate gradually in your abdomen.
Delayed symptoms occur because the body initially compensates for damage. Your cardiovascular system can maintain normal blood pressure even after losing up to 15% of blood volume. Organs continue functioning despite minor tears. Inflammation takes time to develop. By the time symptoms become obvious, the injury has often progressed from manageable to critical.
This delayed timeline creates a dangerous gap where victims feel well enough to skip medical evaluation. They go to bed thinking they dodged serious injury, unaware that internal bleeding continues while they sleep.
Most Common Types of Organ Damage in Motorcycle Accidents
Certain organs suffer disproportionately in motorcycle crashes due to their location, structure, and blood supply. Understanding which organs are most vulnerable helps explain why specific symptoms matter.
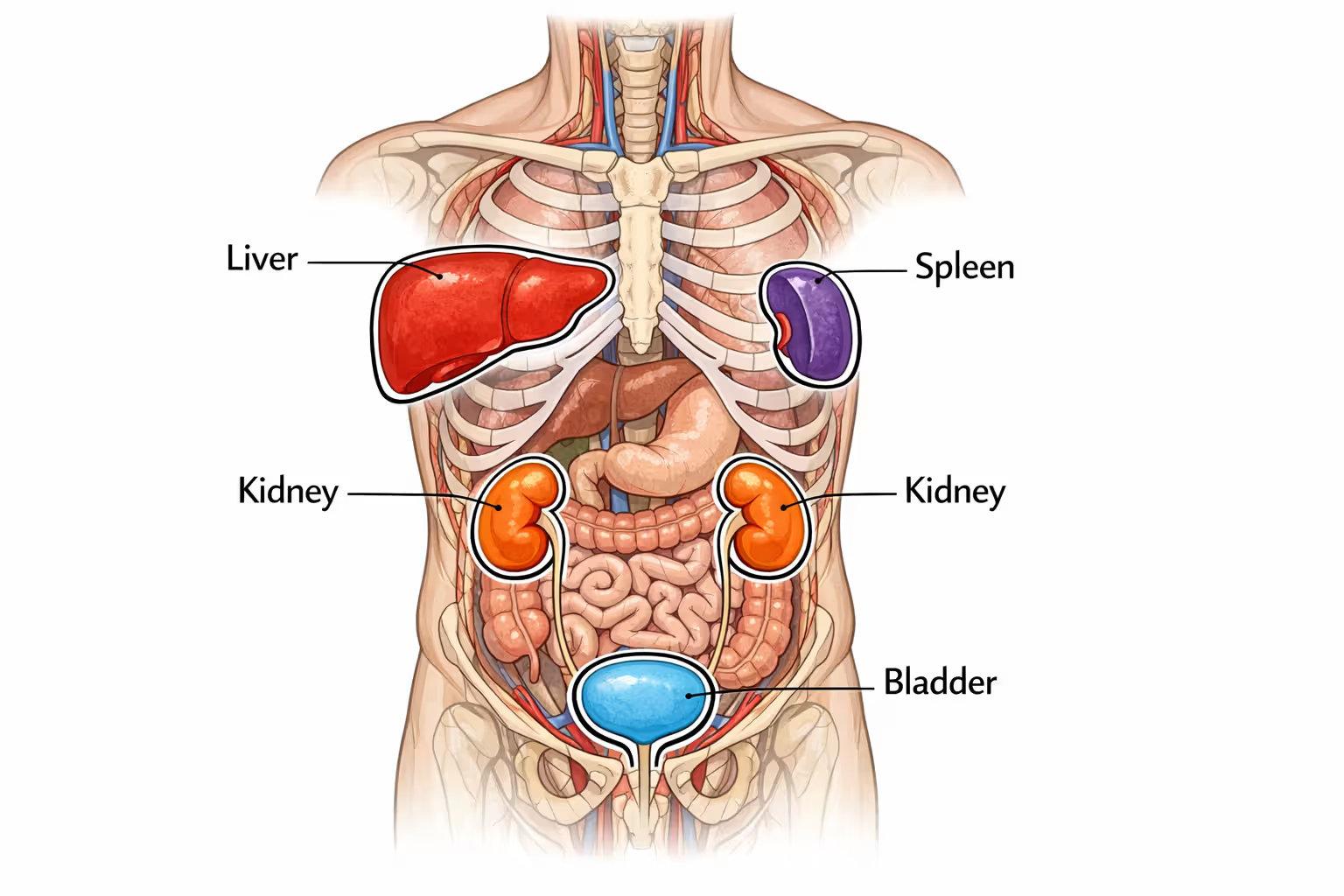
Spleen and Liver Injuries
The spleen and liver sit in your upper abdomen, protected only by the lower ribcage. Both organs are highly vascular—meaning they contain massive blood vessel networks—and both lack the tough, fibrous capsules that protect other organs. When a rider's torso strikes a handlebar, car hood, or pavement, these organs can tear, crack, or rupture completely.
The spleen, located on your left side, is particularly fragile. Even moderate impact can cause a capsular tear that bleeds slowly at first, then ruptures hours later when the damaged tissue gives way. Liver injuries, more common because of the organ's larger size, range from minor lacerations to complete fragmentation in severe crashes.
Both injuries present similar initial symptoms: left or right upper abdominal pain, left shoulder pain (from blood irritating the diaphragm), and progressive weakness as blood loss continues. A person with a damaged spleen might feel fine for six hours, then suddenly deteriorate as delayed bleeding accelerates.
Kidney and Bladder Trauma
The kidneys sit in your back, flanking your spine at roughly waist level. Direct impact to the lower back or flank area—common when a rider is thrown from a bike—can bruise, lacerate, or shatter these organs. Blood in urine is the telltale sign, though it may not appear immediately if the injury doesn't penetrate the collecting system.
Bladder injuries typically occur when the organ is full at the time of impact. A seatbelt-like force across the lower abdomen (from handlebars or a tank) can rupture a distended bladder, spilling urine into the abdominal cavity. This creates a chemical irritation that mimics other abdominal injuries, sometimes delaying correct diagnosis.
Kidney damage often accompanies rib fractures on the back or side. If you have flank pain and broken ribs after a crash, assume kidney involvement until imaging proves otherwise.
Author: Ryan Whitlock;
Source: spy-delhi.com
Lung Contusions and Pneumothorax
Rib fractures don't just hurt—they indicate significant force was transmitted to the chest cavity. That same force bruises lung tissue (pulmonary contusion) or tears the pleural membrane, allowing air to leak into the chest cavity (pneumothorax).
A lung contusion develops over 24 to 48 hours as bruised tissue swells and fills with fluid, progressively reducing oxygen exchange. Initial breathing might feel normal, but respiratory function gradually worsens. A pneumothorax can be immediate or delayed, depending on whether the initial injury created a hole or just weakened tissue that tears later.
Tension pneumothorax—where air accumulates under pressure—represents a true emergency. The trapped air compresses the heart and major blood vessels, reducing cardiac output. Symptoms escalate quickly: severe shortness of breath, rapid heart rate, anxiety, and eventual cardiovascular collapse.
Bowel and Intestinal Perforations
Handlebar injuries create a specific pattern of abdominal trauma. The concentrated force drives abdominal contents backward against the spine, crushing hollow organs like the small intestine, stomach, or colon. These organs can rupture immediately or develop delayed perforations as bruised tissue dies over the following days.
Bowel perforations leak bacteria-laden digestive contents into the sterile abdominal cavity, triggering peritonitis—a life-threatening infection. Early symptoms are vague: mild abdominal discomfort, nausea, low-grade fever. Within 24 to 48 hours, full-blown peritonitis develops with severe pain, high fever, rigid abdomen, and septic shock.
The challenge with bowel injuries is their subtlety. Unlike solid organ injuries that bleed and cause obvious symptoms, hollow organ perforations may produce minimal early signs. A rider might feel "a bit off" for a day or two before suddenly becoming critically ill.
Warning Signs of Internal Bleeding After a Motorcycle Crash
Internal bleeding doesn't always announce itself with dramatic symptoms. The body compensates until it can't anymore, then deteriorates rapidly. Recognizing the progression helps you identify the window when intervention still works.
Immediate symptoms (first two hours) may include: - Abdominal pain or tenderness, especially if it worsens with movement - Pain in the shoulder tip without direct shoulder injury (referred pain from diaphragm irritation) - Chest pain or difficulty breathing deeply - Visible bruising across the abdomen or flanks - Lightheadedness when standing - Rapid heart rate despite resting
Delayed symptoms (2 to 48 hours) often include: - Progressive weakness or fatigue that worsens instead of improving - Increasing abdominal distension (swelling) - Skin becoming pale, cool, or clammy - Persistent nausea or vomiting - Confusion or difficulty concentrating - Decreasing urine output - Blood in urine or stool
The vital signs that matter most are heart rate and blood pressure. A resting heart rate above 100 beats per minute hours after a crash suggests your body is compensating for blood loss. Blood pressure that drops when you stand (orthostatic hypotension) indicates significant volume depletion. If you check your pulse and it's racing while you're lying down resting, something is wrong internally.
One practical rule: if abdominal pain is getting worse instead of better six hours after a crash, you're bleeding internally until proven otherwise. Pain from muscle soreness or bruising improves with rest. Pain from ongoing bleeding intensifies as blood accumulates and irritates tissues.
Abdominal Injuries: What Happens When Impact Meets Your Core
The abdomen contains no bones to protect its contents—just muscle and soft tissue. When a motorcycle's handlebars, tank, or another vehicle strikes this area, the force compresses everything inside against the spine. Think of it like squeezing a water balloon against a wall: something has to give.
Blunt force trauma to the abdomen creates several injury patterns. Solid organs (liver, spleen, kidneys) can crack or fragment. Hollow organs (intestines, stomach, bladder) can burst or tear. Blood vessels can shear away from their attachments. The mesentery—the fan-like tissue that suspends intestines and contains their blood supply—can tear, cutting off circulation to sections of bowel.
Handlebar injuries deserve special mention because they're so common and so dangerous. The concentrated force of a handlebar striking the abdomen creates what trauma surgeons call a "handlebar hernia"—though it's not actually a hernia. The impact drives abdominal contents through the muscle wall, or it crushes organs against the spine. These injuries often involve multiple organ systems simultaneously: pancreas, duodenum, small bowel, and major blood vessels all clustered in the same area.
Seatbelt-equivalent injuries occur when a rider is thrown forward and the tank or handlebars create a restraining force across the lower abdomen, similar to a lap belt in a car crash. This mechanism commonly causes bladder rupture, lumbar spine fractures, and bowel perforations. The visible sign is a horizontal bruise across the lower abdomen—if you see this mark, assume serious internal injury.
The abdominal injury motorcycle accident guide principle that emergency physicians follow is simple: mechanism matters as much as symptoms. A high-speed crash with abdominal impact requires imaging regardless of how the patient feels, because the forces involved make internal injury likely even without obvious symptoms.
Diagnostic Methods Emergency Rooms Use to Detect Hidden Trauma
Modern emergency departments follow standardized protocols for motorcycle crash victims, using a combination of physical examination, imaging, and laboratory tests to identify hidden injuries before they become critical.
The FAST exam (Focused Assessment with Sonography for Trauma) represents the first-line screening tool. This bedside ultrasound takes less than five minutes and checks four areas where blood accumulates after internal injury: around the heart, in the upper right abdomen (liver area), upper left abdomen (spleen area), and pelvis. Free fluid in any of these spaces indicates bleeding that requires immediate intervention.
The FAST exam's limitation is sensitivity—it detects significant bleeding but can miss smaller injuries. A negative FAST doesn't rule out internal trauma; it just means you're not bleeding massively at that moment.
CT scanning remains the gold standard for detecting organ damage in stable patients. Modern trauma protocols use whole-body CT for high-mechanism crashes, scanning from head to pelvis in a single pass. This imaging identifies solid organ lacerations, bowel wall thickening, free air (indicating perforation), active bleeding, and associated fractures.
CT requires IV contrast to highlight blood vessels and organs. The contrast allows radiologists to see "contrast blush"—areas where contrast leaks from damaged vessels, indicating active bleeding. This finding often determines whether a patient needs surgery immediately or can be monitored conservatively.
Physical examination follows specific patterns. The physician palpates all four abdominal quadrants, checking for tenderness, rigidity, or guarding (involuntary muscle tensing). They percuss—tap with fingers—to assess whether the abdomen is filled with air (normal) or fluid (abnormal). They listen for bowel sounds, though their absence isn't reliable for diagnosing injury.
Certain examination findings are particularly concerning: - Seatbelt sign (horizontal bruising across the abdomen) - Abdominal distension - Rigid, board-like abdomen (suggests peritonitis) - Severe tenderness in a specific area - Bruising on the flanks (Grey Turner's sign) or around the umbilicus (Cullen's sign), both indicating retroperitoneal bleeding
Blood work provides indirect evidence of internal injury. Dropping hemoglobin indicates bleeding. Rising white blood cell count suggests tissue damage or infection. Elevated liver enzymes point to liver injury. Blood in the urine confirms kidney or bladder trauma. Lactate levels reflect tissue perfusion—high lactate means tissues aren't getting enough oxygen, often because of blood loss.
Serial examinations matter as much as initial findings. A patient who seems fine initially but develops worsening tenderness, rising heart rate, or dropping blood pressure over several hours is declaring their internal injury through changing clinical signs.

Author: Ryan Whitlock;
Source: spy-delhi.com
Treatment Timeline: From Emergency Response to Full Recovery
The "golden hour" concept—that outcomes improve dramatically when definitive treatment begins within 60 minutes of injury—drives trauma system design. For internal bleeding, this timeline is critical because the body's compensatory mechanisms eventually fail.
Immediate response (0-2 hours) focuses on stabilization and diagnosis. Paramedics establish IV access, administer oxygen, and transport to a trauma center. The emergency department performs primary survey, FAST exam, and obtains imaging. Blood products are prepared if transfusion seems likely.
Treatment decisions branch based on hemodynamic stability. Unstable patients—those with low blood pressure, signs of shock, or massive bleeding on FAST—go directly to the operating room for exploratory surgery. The goal is hemorrhage control: identify bleeding sources, repair or remove damaged organs, and pack injuries that can't be immediately fixed.
Stable patients with identified injuries often enter non-operative management, a modern approach that recognizes many solid organ injuries heal without surgery if bleeding stops on its own. This requires ICU admission with serial abdominal exams, hemoglobin checks every 4-6 hours, and repeat imaging if clinical status changes. Patients remain on strict bed rest, receive nothing by mouth, and get transfused if hemoglobin drops significantly.
The trade-off with non-operative management is that about 10-15% of patients initially managed conservatively eventually require surgery due to delayed bleeding or complications. The benefit is avoiding surgery's risks and recovery time for the 85-90% whose injuries heal spontaneously.
Surgical interventions for internal injuries vary by organ. Spleen lacerations might be repaired or the entire organ removed (splenectomy). Liver injuries are packed with surgical sponges to control bleeding, sometimes requiring repeat operations to remove packing once bleeding stops. Bowel perforations require resection—cutting out the damaged section and reconnecting healthy ends. Kidney injuries often heal with observation, but severe cases need surgical repair or nephrectomy.
Recovery phases extend far beyond hospital discharge. ICU monitoring typically lasts 2-5 days for significant injuries, followed by floor care until patients can eat, walk, and manage pain with oral medications. Total hospitalization ranges from 3-7 days for moderate injuries to weeks for severe trauma requiring multiple surgeries.
Rehabilitation begins in the hospital with physical therapy to prevent deconditioning and breathing exercises to prevent pneumonia. After discharge, activity restrictions typically last 6-8 weeks—no heavy lifting, contact sports, or activities that could re-injure healing organs. Full recovery to pre-injury baseline can take 3-6 months depending on injury severity and complications.
Long-Term Complications and When to Seek Follow-Up Care
Every year I treat motorcycle riders who walked away from crashes, felt fine, and came to the emergency department only when they collapsed at home. By then, they've lost significant blood volume and face much higher surgical risks. The single most important message I can give is this: mechanism of injury predicts internal damage better than how you feel in the first hour. High-speed crashes, especially with abdominal or chest impact, require immediate evaluation regardless of symptoms. Adrenaline lies. CT scans don't
— Dr. Michael Torres
Surviving the initial injury doesn't guarantee an uncomplicated recovery. Several delayed complications can emerge weeks or months after the accident, requiring ongoing vigilance.
Delayed splenic rupture occurs when a subcapsular hematoma (blood trapped under the spleen's outer capsule) suddenly bursts days or weeks after injury. The initial trauma creates a contained bleed that gradually expands until the capsule tears, releasing accumulated blood into the abdomen. This presents as sudden-onset abdominal pain and signs of shock in someone who seemed to be recovering well. It's rare but well-documented, occurring in about 5% of splenic injuries managed non-operatively.
Infection risks increase after any abdominal injury. Bowel perforations, even when surgically repaired, can develop abscesses—pockets of infected fluid that require drainage. Splenectomy patients face lifelong increased susceptibility to certain bacterial infections, requiring vaccination against pneumococcus, meningococcus, and Haemophilus influenzae. Post-splenectomy patients should seek immediate medical attention for any fever over 101°F.
Chronic conditions resulting from organ damage include: - Chronic kidney disease if significant nephron loss occurred - Pancreatic insufficiency or diabetes if pancreatic damage was severe - Intestinal obstruction from adhesions (scar tissue) that form after abdominal surgery - Chronic pain syndromes from nerve damage or persistent inflammation - Post-traumatic stress disorder affecting up to 30% of serious crash survivors
Follow-up imaging is typically scheduled at 6-8 weeks post-injury to confirm healing. Solid organ injuries should show resolution of lacerations and hematomas. Any persistent abnormalities may require extended activity restrictions or additional intervention.

Author: Ryan Whitlock;
Source: spy-delhi.com
Warning signs that require immediate medical attention during recovery include: - New or worsening abdominal pain - Fever over 101°F - Vomiting, especially if persistent or containing blood - Inability to tolerate food or liquids - Yellowing of skin or eyes (jaundice) - Severe fatigue or weakness that worsens instead of improving - Fainting or near-fainting episodes
One often-overlooked aspect of recovery is psychological. Serious injuries create lasting anxiety about riding, driving, or even being a passenger. This represents a normal trauma response, not weakness. Professional counseling helps many survivors process the experience and regain confidence.
Comparison of Internal Injury Symptoms: Immediate vs. Delayed Onset
| Injury Type | Immediate Symptoms (0-2 hours) | Delayed Symptoms (2-48 hours) | Critical Timeline |
| Splenic rupture | Left upper abdominal pain, left shoulder pain, rapid pulse | Progressive weakness, pale skin, abdominal distension, shock symptoms | 6-24 hours for delayed rupture; up to 2 weeks for subcapsular hematoma rupture |
| Liver laceration | Right upper abdominal tenderness, right shoulder pain | Increasing abdominal girth, jaundice (rare), dropping blood pressure | 4-12 hours for significant bleeding; 24-48 hours for biliary complications |
| Bowel perforation | Mild abdominal discomfort, nausea | Severe abdominal pain, fever, rigid abdomen, septic shock | 12-48 hours for peritonitis to develop |
| Kidney trauma | Flank pain, visible blood in urine | Continued hematuria, flank mass, fever if infection develops | 6-24 hours for expanding hematoma; days to weeks for delayed complications |
| Pneumothorax | Chest pain, shortness of breath (if large) | Progressive breathing difficulty, rapid heart rate, anxiety | Minutes to hours for tension pneumothorax; 24-72 hours for delayed pneumothorax |
Frequently Asked Questions
Conclusion
The rider who walks away from a crash isn't always the lucky one—sometimes they're just on a delayed timeline. Internal injuries from motorcycle accidents kill people who survive the initial impact because hidden damage progresses silently until it reaches a crisis point.
Your best protection is knowledge and action. Understand that high-force crashes cause internal injuries regardless of how you feel immediately afterward. Recognize that adrenaline masks pain and that the most dangerous injuries often produce the subtlest early symptoms. Know that abdominal pain worsening over hours, progressive weakness, rapid pulse, and shoulder pain without shoulder injury all indicate internal bleeding.
Most importantly, seek immediate medical evaluation after any significant motorcycle crash. The inconvenience of an emergency department visit pales compared to the consequences of missed internal trauma. Modern imaging can identify injuries while they're still manageable, before bleeding becomes massive or infection becomes systemic.
If you've been in a motorcycle accident, even if you feel fine right now, consider this your permission to take internal injuries seriously. Call for medical evaluation. Accept ambulance transport if offered. Undergo recommended imaging. Stay for observation if advised. These decisions could save your life by catching hidden trauma before it becomes a catastrophe.
Your body absorbed enormous forces in that crash. Respect what that means for your internal organs, even when your external appearance suggests you escaped unscathed. The life you save by seeking evaluation might be your own.
Related Stories

Read more

Read more




The content on this website is provided for general informational and educational purposes only. It is intended to offer insights and guidance on motorcycle accident insurance claims, settlement processes, liability issues, coverage limits, medical compensation, and related insurance matters, and should not be considered legal or financial advice.
All information, articles, and materials presented on this website are for general informational purposes only. Insurance policies, liability standards, settlement practices, and state regulations may vary by jurisdiction and insurer. The outcome of a motorcycle accident claim depends on the specific facts of the accident, available evidence, policy language, and applicable law.
This website is not responsible for any errors or omissions in the content, or for actions taken based on the information provided. Users are strongly encouraged to consult with a qualified attorney or licensed insurance professional regarding their specific motorcycle accident claim before making decisions about settlements, negotiations, or coverage disputes.