

Motorcyclist riding on urban road at dusk with focus on exposed neck area between helmet and leather jacket highlighting vulnerability
Motorcycle Accident Neck Injury Guide to Diagnosis, Treatment, Recovery

Here's what most riders don't realize until it's too late: your helmet protects your skull, but your neck? It's on its own. When metal meets pavement at 40 mph, your head—10 to 12 pounds of weight balanced on seven small vertebrae—becomes a wrecking ball. Car drivers get airbags, crumple zones, and seatbelts. You get ejected, tumbling across asphalt with nothing between your cervical spine and catastrophic injury except luck and maybe a good leather jacket.
The choices you make right after a crash matter more than you'd think. Which emergency room you visit, whether you insist on imaging, how quickly you start treatment—these decisions separate riders who heal completely from those nursing chronic pain years later. And here's the frustrating part: insurance adjusters know exactly which mistakes to exploit.
How Motorcycle Crashes Cause Neck Injuries
Impact Forces and Biomechanics
Picture this: you're riding 35 mph when a car turns left across your lane. You hit the brakes. The bike stops. Your body? Still traveling at original speed until something interrupts that momentum—usually the pavement, a guardrail, or another vehicle. Your head snaps forward with enough force to tear ligaments that took millions of years of evolution to strengthen.
Engineers call this differential deceleration. Your torso decelerates first while your head keeps moving, creating shear forces across every structure connecting them. Those seven cervical vertebrae, the spinal cord threading through them, the discs cushioning each segment, the muscles holding everything together—all simultaneously stretched beyond their design limits.
Front-end crashes force your chin toward your chest. Your forehead might hit the handlebars. The front of your neck compresses while ligaments along the back stretch and tear. Rear impacts do the opposite—your head whips backward, potentially driving the spinal cord against the back of the vertebral canal. Side impacts add rotation, and the cervical spine handles twisting forces about as well as you'd expect from a structure built for nodding and looking side to side, not spinning like a top.
Speed determines severity, obviously. But so does body position at impact, whether you tensed your neck muscles beforehand (riders who see the crash coming often fare worse because tense muscles transmit more force), your age, previous neck problems, and pure chance.

Author: Caleb Thornton;
Source: spy-delhi.com
Why Motorcyclists Face Higher Risk Than Car Occupants
Cars are mobile safety cages. The frame absorbs energy. Airbags deploy. Seatbelts distribute forces across your strongest bones. You might walk away from a 45 mph crash with nothing worse than bruises.
Hit something at 45 mph on a bike? You're probably airborne, and you'll land on whatever body part hits first—often your head and shoulders. No frame to crumple. No airbag to catch you. Your body absorbs 100% of the kinetic energy.
Some trauma surgeons talk about "helmet amplification"—the extra weight and size of a helmet can actually increase rotational forces during tumbling impacts. Does this mean skip the helmet? Absolutely not. Helmets prevent fatal brain injuries. But they're not neck protection. That's a separate problem requiring separate solutions (like airbag vests, though adoption remains low).
National Highway Traffic Safety Administration data shows motorcyclists suffer cervical injuries four to six times more frequently than car occupants in equivalent-speed collisions. The human neck simply wasn't designed to be the primary impact-absorption system.
Common Types of Neck Injuries After a Motorcycle Accident
Whiplash and Soft Tissue Damage
Insurance adjusters love dismissing whiplash as "just a sprain." Tell that to someone three months post-crash who still can't turn their head enough to check a blind spot. Whiplash involves thousands of microscopic tears through muscles, tendons, and ligaments—tissue damage invisible on X-rays but producing very real pain.
The injury mechanism is straightforward: soft tissues stretch past their elastic limit, triggering inflammation. Your body responds by splinting the area with muscle spasms, which ironically makes everything hurt worse. Scar tissue forms in random patterns. Without proper treatment, you end up with permanent stiffness.
Symptoms usually appear 24 to 72 hours post-crash: neck stiffness that makes parking a nightmare, pain spreading into shoulders, headaches starting where your skull meets your spine, difficulty concentrating (yes, neck injuries affect cognition). Some riders experience vertigo, TMJ problems, or that annoying "fog brain" feeling.
Here's the concerning statistic: about 15-20% of whiplash patients develop chronic symptoms lasting beyond six months. The common denominator? Inadequate early treatment or rushing back to normal activities before tissues heal.
Cervical Fractures and Dislocations
High-speed impacts break bones. The cervical vertebrae—those seven knobby segments forming your neck—can fracture in several distinct patterns, each with its own name and nightmare scenario:
Compression fractures happen when you land headfirst. The vertebral body—the round front part bearing most weight—collapses like a crushed soda can. If the back portion stays intact, the spine remains relatively stable. If not, bone fragments can shift into the spinal canal.
Hangman's fractures involve bilateral breaks through C2's arch. Despite the grim name (yes, it's the same fracture pattern hanging produces), many heal well with immobilization. The mechanism requires sudden hyperextension combined with compression—think getting rear-ended while looking up.
Jefferson fractures burst the C1 ring outward. C1, the atlas vertebra, supports your skull. Axial loading—vertical compression from helmet-first impacts—can split it into multiple fragments. This injury destabilizes the skull-spine junction, which is about as serious as it sounds.
Odontoid fractures break the peg on C2 that acts as a pivot point for head rotation. Type I fractures (tip only) heal fine. Type II fractures (base of the peg) often fail to heal without surgery. Type III fractures (extending into C2 body) are stable but require months in a halo.
Dislocations mean vertebrae slip out of alignment. Partial displacement (subluxation) tears ligaments but may spontaneously reduce. Complete dislocations almost always damage the spinal cord unless reduced immediately. Without surgery, these injuries leave the spine unstable even after bones heal—imagine trying to balance a tower of blocks with rubber bands instead of mortar.
Spinal Cord Injuries
The spinal cord—about as thick as your thumb—carries every nerve signal between your brain and body. It runs through a bony tunnel formed by your vertebrae. When fractures narrow that tunnel, or when dislocated vertebrae pinch the cord, or when disc material herniates backward into the canal, the results range from temporary numbness to permanent quadriplegia.
A complete spinal cord injury severs all nerve pathways. Everything below the injury level goes silent—no sensation, no movement, no autonomic control. Incomplete injuries spare some nerve tracts, allowing partial function, though "partial" covers a massive range from "slightly weak grip" to "can't walk but can wiggle toes."
Cervical cord injuries are the most devastating. Damage at C1-C4 paralyzes the diaphragm, requiring permanent ventilation. C5-C7 injuries might preserve shoulder and elbow function but eliminate hand control and everything below the waist. Even "minor" cord contusions produce central cord syndrome—a weird pattern where hands become weaker than legs, with burning pain and lost fine motor skills. This happens because nerve fibers controlling the arms run through the cord's center, which sustains more damage during compression.
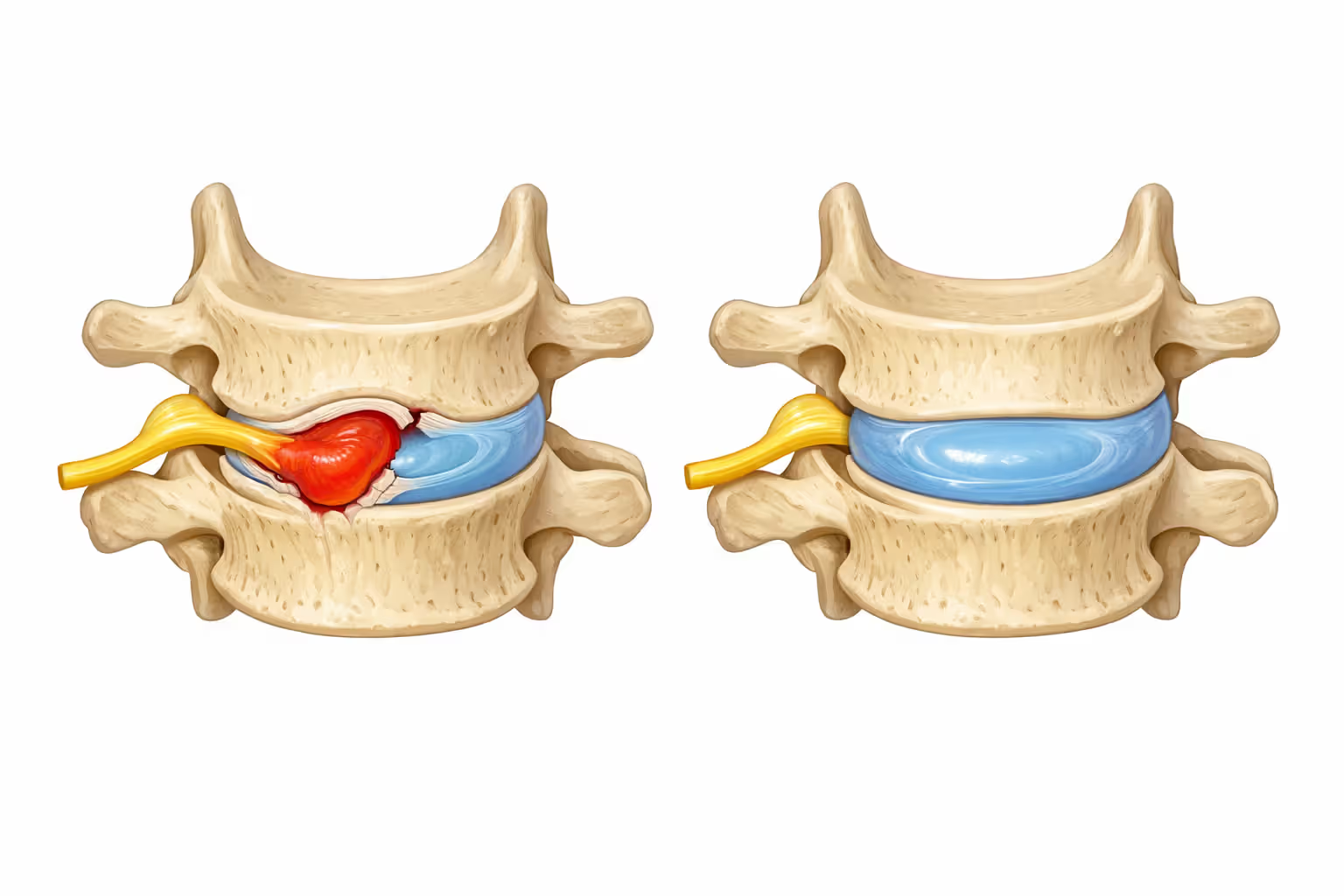
Herniated Discs in the Cervical Spine
Think of intervertebral discs as jelly donuts sandwiched between vertebrae. The outer part (annulus fibrosus if we're being technical) is tough, layered cartilage. The center (nucleus pulposus) is gelatinous material that squishes and rebounds to absorb shocks.
Trauma tears the outer layers, letting the jelly squeeze out. When disc material pushes sideways, it compresses nerve roots exiting the spinal cord. This is radiculopathy—electric, shooting pain down your arm, numbness in specific fingers, weakness in particular muscles. Which fingers go numb tells doctors exactly which disc herniated: C6-C7 affects thumb and index finger, C7-T1 hits the pinky side.
Large herniations pushing straight backward compress the spinal cord itself, causing myelopathy. Symptoms include wobbly walking, fumbling with keys, bladder dysfunction, and widespread numbness. This qualifies as a surgical emergency—decompression within days prevents permanent disability.
Author: Caleb Thornton;
Source: spy-delhi.com
Warning Signs You Shouldn't Ignore After a Motorcycle Crash
Adrenaline is a liar. Right after impact, you might feel invincible. You'll walk around, talk to police, refuse the ambulance because you "feel fine." Then you wake up the next morning unable to lift your head off the pillow.
This delay isn't psychological. Inflammation takes hours to develop. Swelling progresses over days. Muscle spasms intensify as your body realizes something's wrong. Some herniated discs take 48 hours to swell enough to compress nerves.
Get to an emergency room immediately if you notice:
- Severe neck pain or complete inability to move your head
- Numbness, tingling, or weakness anywhere below your neck
- Lost bladder or bowel control (sign of cauda equina syndrome)
- Trouble breathing or swallowing
- Confusion, vision changes, or severe headache
- Pain radiating down both arms simultaneously
These symptoms suggest cord compression, unstable fractures, or associated traumatic brain injury. Time matters—a lot.
Visit urgent care or your doctor within 24 hours for:
- Moderate neck pain or stiffness (pain level 4-7 out of 10)
- Headaches getting progressively worse
- Shoulder or upper back pain
- Brain fog, memory problems, or difficulty concentrating
- Nausea or dizziness when moving your head
Even seemingly minor symptoms deserve evaluation. Insurance companies will later argue that delayed treatment proves injuries weren't serious. More importantly, some cervical injuries worsen without proper immobilization.
Monitor yourself for delayed symptoms over two weeks:
- Pain intensity gradually increasing instead of improving
- New numbness or tingling appearing days later
- Tasks that were easy suddenly becoming difficult
- Can't sleep due to pain or can only sleep in certain positions
- Irritability or mood changes (often indicates chronic pain)
Document everything. Snap photos of bruises, swelling, any visible injuries. Keep a symptom journal with dates and specific descriptions. This record becomes crucial for medical treatment decisions and any legal claim you might pursue.

Author: Caleb Thornton;
Source: spy-delhi.com
Diagnostic Tests Doctors Use to Evaluate Neck Trauma
Emergency responders assume the worst—they'll collar and backboard you before transport. At the hospital, physicians follow a systematic approach combining hands-on examination with imaging.
The physical exam covers:
- Palpating your neck for tender spots, swelling, gaps, or deformity
- Testing range of motion (only if fracture is ruled out first)
- Neurological checks: can you squeeze hands equally? Do your reflexes work? Can you feel a pin prick on both sides?
- Looking for associated injuries since motorcycle crashes rarely involve just one body part
Imaging reveals what hands can't feel:
Imaging Method Comparison for Diagnosing Neck Injuries
| Imaging Type | What It Reveals | Primary Uses | Cost Estimate | Radiation Level |
| X-ray | Bone position, obvious breaks, alignment, vertebral spacing | First screening step for fractures and dislocations | $100-$300 | Low (0.2 mSv) |
| CT Scan | Three-dimensional bone detail, small fracture lines, fragment locations | Confirming suspected fractures, planning surgery, evaluating unstable injuries | $500-$1,500 | Moderate (3-6 mSv) |
| MRI | Soft tissue structures including discs, ligaments, spinal cord, nerve roots | Identifying herniated discs, cord compression, torn ligaments | $1,000-$3,000 | None |
| Ultrasound | Real-time soft tissue movement, blood flow assessment | Rarely used except for guiding injections | $200-$500 | None |
X-rays come first. Three standard views (side, front, and through-the-mouth to see C2) catch most fractures and dislocations. But X-rays are essentially bone pictures—they miss soft tissue damage, small fractures, and spinal cord problems entirely.
CT scans provide three-dimensional bone detail with submillimeter resolution. Radiologists can digitally reconstruct images from any angle, essential for understanding complex fracture patterns before surgery. CT is unmatched for diagnosing cervical fractures, though it exposes you to significantly more radiation than X-rays.
MRI reveals everything bones hide: spinal cord bruising, bulging discs, torn ligaments, nerve root inflammation. Doctors order MRIs when you have neurological symptoms, persistent pain despite normal X-rays, or when considering surgery. The downside? MRIs take 30-60 minutes lying motionless inside a noisy, claustrophobic tube—challenging when your neck is screaming.
Some facilities perform flexion-extension radiographs several days post-injury to detect instability. You carefully bend your neck forward and backward while technicians capture images showing whether vertebrae move abnormally. This test remains controversial because asking injured patients to move their neck could theoretically worsen unstable injuries.
Treatment Options: From Emergency Care to Long-Term Recovery
Immediate Medical Interventions
Paramedics immobilize your cervical spine before moving you. Emergency physicians "clear" the spine through examination and imaging before removing the collar. For unstable fractures or dislocations, immediate interventions include:
Cervical traction: Weights attached to tongs screwed into your skull (yes, really) or a halo device gradually pull misaligned vertebrae back into position. This reduces dislocations and relieves pressure on the spinal cord before surgery. You'll lie flat for hours or days while weights incrementally increase.
Halo vest immobilization: A metal ring literally bolts to your skull via four titanium pins, then connects to a rigid vest encasing your torso. This completely immobilizes your head relative to your body. Patients wear halos for 8-12 weeks while fractures heal—no driving, no showers without help, sleeping upright in a recliner. It's miserable but effective.
Emergency decompression surgery: Spinal cord compression doesn't wait for scheduled surgery. Surgeons remove bone fragments, herniated disc material, or blood clots pressing on neural tissue, often simultaneously stabilizing the spine with plates and screws.
High-dose methylprednisolone: This steroid protocol was standard for acute cord injuries for decades. Recent evidence shows minimal benefit with potential complications (infections, bleeding, blood sugar problems), so many trauma centers abandoned it. Your hospital might still offer it within eight hours of injury.
Conservative Treatments (Physical Therapy, Medications, Bracing)
Most soft tissue injuries and stable fractures heal without surgery. Conservative approaches focus on controlling pain, preventing stiffness, and gradually rebuilding function.
Cervical collars: Soft foam collars provide comfort and remind you to limit motion, but they don't truly stabilize anything. Rigid collars offer better support for stable fractures. Here's the catch: wearing a collar beyond 2-3 weeks weakens neck muscles through disuse. Doctors balance protection against deconditioning.
Medications: NSAIDs (ibuprofen, naproxen, meloxicam) reduce inflammation and provide pain relief without the addiction risks of opioids. Muscle relaxants like cyclobenzaprine or methocarbamol address painful spasms. Severe pain might require short-term opioids, though physicians now prescribe them cautiously—usually no more than a week or two. Nerve pain responds better to gabapentin or pregabalin than traditional painkillers.
Physical therapy: Once acute pain subsides (usually within a week), physical therapists guide you through exercises restoring motion, strength, and posture. Early mobilization prevents chronic stiffness—the neck needs controlled movement to heal properly. Therapists employ manual therapy, mechanical traction, ultrasound, electrical stimulation, and progressive exercises tailored to your specific injury.
Here's what most patients don't understand: staying immobile too long guarantees chronic problems. Neck muscles atrophy within days. Scar tissue forms in shortened positions, cementing permanent stiffness. For typical whiplash injuries, we're starting gentle range-of-motion exercises within the first week—even while patients still have significant pain. Movement is medicine
— Dr. Michael Torres
Therapeutic injections: Trigger point injections deliver local anesthetic and corticosteroid directly into painful muscle knots, providing relief for days or weeks. Epidural steroid injections target inflamed nerve roots compressed by herniated discs. Facet joint injections address arthritis in the small joints connecting adjacent vertebrae. These interventions provide temporary relief, creating a window for healing and rehabilitation to progress.
Surgical Procedures for Severe Cervical Injuries
Surgery becomes necessary when the spinal cord or nerve roots face compression, when fractures prove unstable or displaced, when conservative treatment fails after 6-12 weeks, or when discs herniate causing progressive neurological problems.
Anterior cervical discectomy and fusion (ACDF): Surgeons approach through the front of your neck (they temporarily move your esophagus and trachea aside—don't think about it too much), remove the damaged disc, and insert a spacer filled with bone graft material between vertebrae. A titanium plate screwed to both vertebrae holds everything rigid while fusion occurs over 3-6 months. This decompresses pinched nerves and creates permanent stability.
Posterior cervical fusion: Approaching from behind your neck, surgeons connect vertebrae using rods and screws, immobilizing unstable segments. This technique works well for fractures, dislocations, and injuries involving multiple levels.
Artificial disc replacement: Instead of fusing vertebrae into one immobile block, surgeons implant a mobile prosthetic disc preserving motion. This newer option theoretically reduces adjacent segment degeneration—arthritis developing above and below fused levels due to increased stress. Long-term data (20+ years) remains limited compared to fusion.
Laminectomy with or without fusion: Removing part of the vertebral arch (lamina) expands space available for the spinal cord. This decompresses stenosis or herniations compressing the cord from behind. If ligaments get removed, surgeons add fusion to prevent instability.
Recovery from cervical spine surgery typically requires 6-12 weeks in a collar, followed by several months of physical therapy. Fusion surgeries successfully relieve arm pain and prevent paralysis in 85-95% of cases, though improvement in neck pain itself is less predictable—some patients trade nerve pain for fusion-related stiffness.

Author: Caleb Thornton;
Source: spy-delhi.com
Recovery Timeline: What to Expect During Neck Injury Rehabilitation
Recovery varies dramatically based on what got injured, how severely, your age, overall health, and whether you consistently follow treatment recommendations.
Minor whiplash (Grade I-II soft tissue strain): - First 1-2 weeks: Acute pain and stiffness; gentle range-of-motion exercises start almost immediately - Weeks 3-6: Pain decreases substantially; physical therapy becomes more intensive - Weeks 6-12: Most riders return to normal activities including riding - Persistent symptoms beyond 12 weeks affect 10-15% of patients, requiring ongoing management
Moderate soft tissue injuries (Grade III sprains with torn ligaments): - Weeks 1-4: Wearing a collar, managing pain, limited activity - Months 2-3: Progressive physical therapy, gradual return to work with restrictions - Months 3-6: Continued improvement though some residual stiffness is common - Full recovery typically takes 6-12 months
Stable cervical fractures: - Weeks 1-8: Rigid collar or halo vest immobilization - Weeks 8-12: Collar removed after X-rays confirm healing; cautious physical therapy begins - Months 3-6: Strengthening exercises, gradual increase in activities - Months 6-12: Most patients regain full or near-full function, though some experience chronic discomfort
Surgical cases (fusion or disc replacement): - Weeks 1-2: Hospital stay for pain control and wound healing - Weeks 2-6: Wearing collar at home, walking encouraged, zero lifting or bending - Weeks 6-12: Collar removed once imaging shows adequate healing; therapy begins - Months 3-6: Progressive strengthening, return to most activities - Months 6-12: Fusion solidifies on imaging; functional recovery mostly complete - Full recovery including complete fusion often takes 12-18 months
Spinal cord injuries: - Outcomes depend entirely on whether the injury is complete or incomplete, and at what level - Maximum recovery typically occurs within the first six months - Intensive rehabilitation continues 12-24 months - Incomplete injuries may show gradual improvement for years - Complete injuries (total cord transection) rarely recover function below the injury level
Recovery gets slower with age—tissues heal less efficiently after 50. Smoking dramatically impairs healing by restricting blood flow (it also increases fusion failure rates). Poor nutrition lacking adequate protein and vitamins delays tissue repair. Obesity increases mechanical stress on healing structures. Delayed treatment allows inflammation and abnormal scar tissue formation to establish chronic pain patterns. Inadequate physical therapy results in permanent stiffness. Psychological factors including depression and anxiety amplify pain perception. Some studies even suggest symptom resolution accelerates after legal claims settle, though whether this represents malingering or stress reduction remains debated.
Mistakes That Can Worsen Your Neck Injury or Damage Your Claim
Skipping or delaying medical evaluation: Two problems here. First, insurance adjusters will argue that treatment gaps prove injuries weren't serious—they'll hire doctors to testify that real injuries cause immediate pain requiring immediate care. Second, and more important, untreated fractures can shift out of position, and disc herniations can progressively worsen, causing irreversible nerve damage. Get evaluated within 24 hours even if you're convinced you're fine.
Ignoring treatment recommendations: Missing physical therapy appointments, not taking prescribed medications, or removing your collar early extends recovery and hands insurance companies ammunition to deny your claim. They'll argue you didn't follow medical advice, so any persistent problems are your fault. If a treatment isn't working or causes problems, discuss alternatives with your physician rather than just stopping.
Grabbing quick settlement offers: Adjusters often call within days offering fast settlements before you understand injury severity. Neck injuries frequently worsen weeks post-crash. Chronic pain may not develop for months. Once you sign that release accepting $5,000, you can't reopen the claim when you discover you need $50,000 in surgery six months later.
Failing to document symptoms: Start a daily journal immediately. Record pain levels (0-10 scale), which activities hurt, medications taken, appointments attended, and how injuries affect daily life. Photograph visible injuries like bruising or swelling. Take photos of your collar, brace, or any assistive devices. This documentation proves injury severity when the adjuster claims you're exaggerating.
Social media posting during recovery: That photo of you hiking—even if it's gentle therapeutic walking recommended by your doctor—will get screenshot and presented as proof you're lying about your injuries. Adjusters routinely monitor claimants' social media. Set everything to private and don't post anything about your accident, injuries, or activities until your claim resolves.
Delaying attorney consultation: Statutes of limitation vary by state (typically 2-3 years for personal injury) but evidence deteriorates quickly. Witnesses forget details. Accident scene conditions change. Medical records become harder to obtain. Consult an attorney early even if you're unsure about pursuing a claim—initial consultations are usually free.
Returning to work or riding too soon: Financial pressure often forces early return, but pushing through pain risks re-injury and chronic problems that never fully heal. Discuss modified duty options with your employer. Many riders face psychological pressure to "be tough"—resist this. Healing takes time whether you acknowledge it or not.
Ignoring psychological symptoms: Post-traumatic stress, depression, and anxiety commonly follow serious crashes. These conditions are legitimate injuries deserving treatment. They also complicate physical recovery—chronic pain and psychological distress form a vicious cycle. Mental health treatment is essential, not optional, and it's compensable in injury claims.
Frequently Asked Questions About Motorcycle Accident Neck Injuries
Conclusion
Motorcycle accident neck injuries span a spectrum from temporary muscle strains healing in weeks to catastrophic spinal cord damage causing permanent paralysis. The combination of high-impact forces and minimal neck protection makes cervical injuries frighteningly common among crashed riders. Recognizing warning signs, pursuing prompt medical evaluation, obtaining appropriate imaging, and consistently following treatment recommendations dramatically improve your chances of complete recovery.
Don't minimize symptoms or delay care thinking you're tough enough to power through. Inflammation and structural damage take time to manifest—feeling okay immediately after a crash means nothing. Document everything from day one, follow your treatment plan religiously, and avoid common mistakes that jeopardize both your physical recovery and potential compensation.
Recovery timelines range from weeks for minor whiplash to months for surgically repaired fractures, with most patients regaining substantial function through proper treatment and dedicated rehabilitation. Understanding your specific injury type, available treatment options, and realistic recovery expectations helps you make informed decisions during what is undoubtedly one of the most challenging periods of your life.
Related Stories

Read more

Read more




The content on this website is provided for general informational and educational purposes only. It is intended to offer insights and guidance on motorcycle accident insurance claims, settlement processes, liability issues, coverage limits, medical compensation, and related insurance matters, and should not be considered legal or financial advice.
All information, articles, and materials presented on this website are for general informational purposes only. Insurance policies, liability standards, settlement practices, and state regulations may vary by jurisdiction and insurer. The outcome of a motorcycle accident claim depends on the specific facts of the accident, available evidence, policy language, and applicable law.
This website is not responsible for any errors or omissions in the content, or for actions taken based on the information provided. Users are strongly encouraged to consult with a qualified attorney or licensed insurance professional regarding their specific motorcycle accident claim before making decisions about settlements, negotiations, or coverage disputes.