

Motorcycle rider on wet asphalt after crash with focus on injured knee area and fallen motorcycle in background
Motorcycle Accident Knee Injury – Types, Treatment, Recovery Guide

Motorcycle crashes expose riders to unique injury patterns. While helmets protect the head and jackets shield the torso, knees often absorb tremendous force during impact. Whether striking the pavement, colliding with another vehicle, or twisting unnaturally as the bike goes down, the knee joint faces multiple trauma vectors simultaneously.
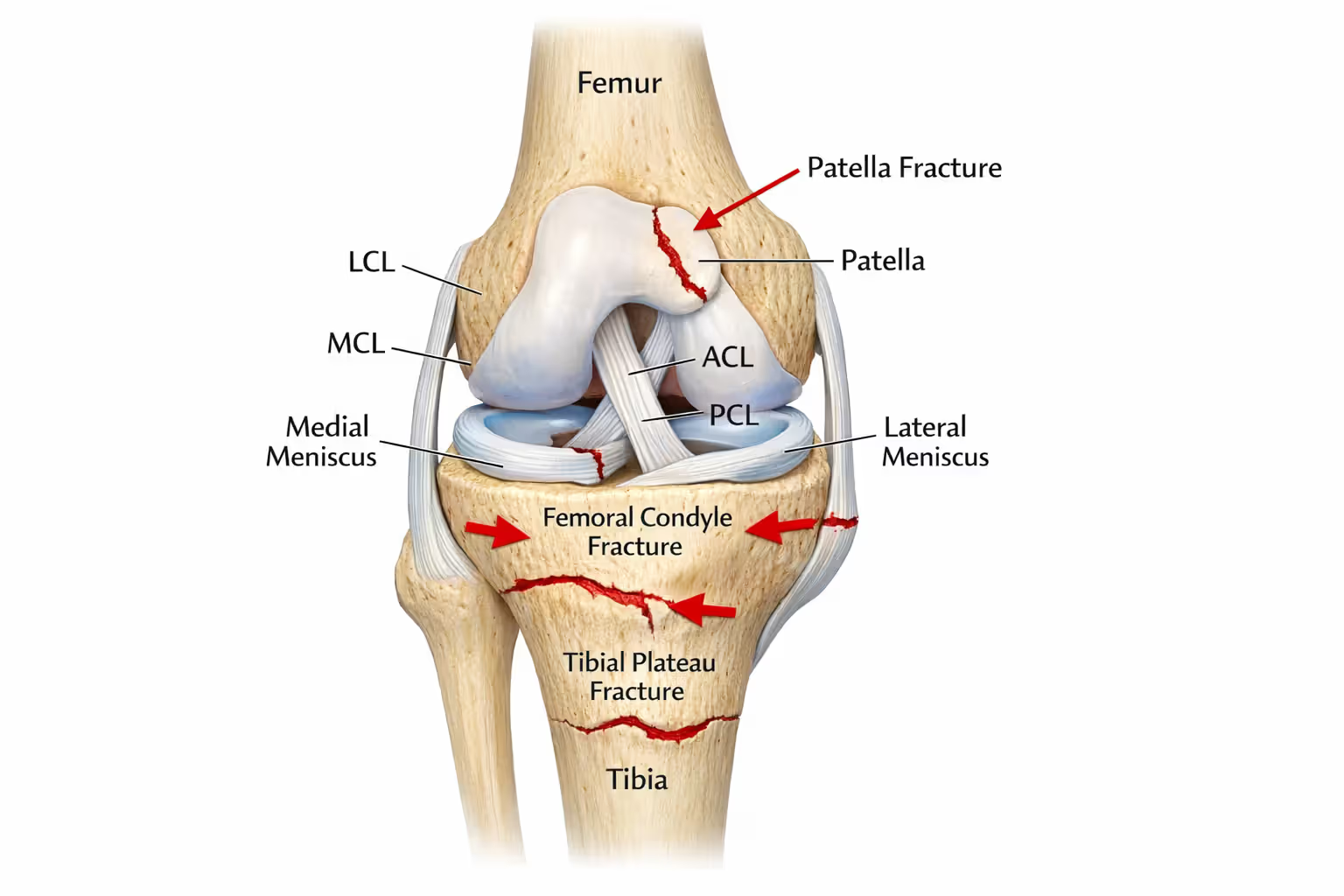
The knee's complex anatomy—four major ligaments, two menisci, cartilage surfaces, and surrounding soft tissue—makes it vulnerable to several injury types at once. A single crash can tear an ACL, fracture the patella, and shred skin in one devastating moment. Understanding what happened inside your knee, what treatment you need, and how long recovery takes can help you make informed decisions during a stressful time.
Common Types of Knee Injuries from Motorcycle Crashes
Ligament Tears (ACL, MCL, PCL)
The anterior cruciate ligament (ACL) tears when the knee hyperextends or rotates violently—common when a rider's leg gets trapped between the bike and pavement. ACL injuries rarely occur alone in motorcycle crashes. You'll often see a combined ACL and MCL tear, or the "unhappy triad" that includes meniscus damage.
MCL (medial collateral ligament) injuries happen when force strikes the outer knee, pushing it inward. This occurs frequently when another vehicle hits the motorcycle from the side. MCL tears range from Grade I (mild stretch) to Grade III (complete rupture). Grade I and II tears typically heal without surgery, while Grade III often requires reconstruction.
PCL (posterior cruciate ligament) tears are less common but occur when the front of the knee slams into something during impact—like the gas tank or another vehicle. Dashboard knee injuries in cars follow similar mechanics. PCL tears cause instability when walking downhill or descending stairs.
The LCL (lateral collateral ligament) on the outer knee tears when force pushes the knee outward. This injury is less frequent but creates significant instability when it happens.
Fractures and Bone Damage
Patella fractures occur when the kneecap strikes the pavement or dashboard. These fractures fall into several categories: transverse (horizontal break), comminuted (shattered into pieces), or avulsion (ligament pulls bone fragment away). Displaced fractures—where bone pieces separate—almost always require surgery. Non-displaced fractures may heal with immobilization.
Tibial plateau fractures affect the top of the shinbone where it meets the femur. These fractures damage the weight-bearing surface of the knee joint. Because this area is mostly cancellous (spongy) bone, it can collapse under impact, creating depression fractures. Surgeons often need to elevate the collapsed bone and support it with bone graft and metal plates.
Femoral condyle fractures involve the rounded ends of the thighbone. High-energy motorcycle crashes can shear these condyles or create T-shaped or Y-shaped fractures that split the femur vertically. These injuries require precise surgical reconstruction to restore joint alignment.
Author: Hannah Pierce;
Source: spy-delhi.com
Meniscus and Cartilage Injuries
The menisci are C-shaped cartilage pads that cushion the knee joint. Twisting injuries during a crash can tear them radially (like spokes on a wheel), horizontally (splitting top from bottom), or create bucket-handle tears where a large fragment flips into the center of the joint. Bucket-handle tears lock the knee, preventing full extension.
Meniscus tears in motorcycle accidents often accompany ligament injuries. The outer third of each meniscus has blood supply and can heal; the inner two-thirds lack blood flow and won't heal without surgical intervention.
Articular cartilage—the smooth surface covering bone ends—can shear off during impact, creating loose bodies that float in the joint. These fragments cause catching, locking, and sudden pain. Cartilage damage also occurs when fractures disrupt the joint surface, leading to post-traumatic arthritis years later.
Soft Tissue Trauma and Road Rash
Road rash on the knee ranges from superficial abrasions to deep wounds exposing muscle, tendon, or bone. Deep road rash introduces bacteria and debris into the wound, creating infection risk. Wounds over joints are particularly problematic because knee flexion constantly reopens healing tissue.
Degloving injuries occur when friction tears skin and fat away from underlying tissue. These injuries may look deceptively minor externally but have extensive damage underneath. Blood supply to the skin is compromised, leading to tissue death if not treated aggressively.
Prepatellar bursitis (fluid accumulation in front of the kneecap) can develop after direct impact. While not immediately serious, chronic bursitis causes ongoing pain and swelling.
Motorcycle knee injuries present unique challenges because riders often sustain multiple injury types simultaneously. We frequently see a combination of ligament tear, fracture, and significant soft tissue damage—what we call the 'motorcycle knee complex.' Each component requires specific treatment, and the soft tissue damage often dictates surgical timing more than the structural injuries themselves
— Dr. Michael Chen
How to Recognize Serious Knee Trauma After a Motorcycle Accident
Immediate post-crash adrenaline masks pain. Riders sometimes walk away from crashes, only to collapse minutes later when adrenaline wears off. Certain symptoms demand immediate emergency evaluation.
Immediate red flags:
Visible deformity means something is fractured, dislocated, or completely torn. If your knee looks wrong—bent sideways, kneecap shifted, or obviously swollen within minutes—you need emergency imaging.
Inability to bear weight suggests significant structural damage. Some people can't put weight down due to pain; others physically can't because the knee buckles or gives way. Both scenarios require evaluation.
Rapid swelling (within two hours) indicates bleeding inside the joint. Blood accumulates faster than other fluids, so rapid swelling suggests torn ligaments, fractures, or both. A knee that swells dramatically overnight is concerning but less urgent than one that balloons in an hour.
Numbness or tingling below the knee indicates potential nerve or vascular damage. The peroneal nerve wraps around the outer knee and can be stretched or torn during impact. Damage to this nerve causes foot drop—inability to lift your foot upward.
Cold foot or absent pulse suggests vascular injury. The popliteal artery runs behind the knee and can tear during dislocations or certain fractures. This is a surgical emergency; permanent damage occurs within hours.

Author: Hannah Pierce;
Source: spy-delhi.com
Delayed symptoms appearing hours or days later:
Stiffness that progressively worsens suggests ongoing inflammation or developing scar tissue. Some stiffness is normal, but you should be able to bend your knee at least 90 degrees within a few days unless you have a specific injury preventing it.
Locking or catching sensations indicate loose bodies or meniscus tears. Your knee may suddenly refuse to straighten, requiring manipulation to unlock.
Instability—feeling like your knee will give out—suggests ligament damage. You might notice this when pivoting, going down stairs, or walking on uneven ground.
Persistent swelling beyond one week indicates continued inflammation, possible infection, or ongoing internal damage.
Diagnostic Tests Your Doctor Will Order
Physical examination comes first. Your doctor will assess range of motion, stability, and specific pain locations. The Lachman test checks ACL integrity, the valgus/varus stress test evaluates collateral ligaments, and the McMurray test detects meniscus tears. However, pain and swelling often prevent accurate physical examination immediately after injury.
| Imaging Method | What It Shows | Time Required | Cost Range | When It's Used |
| X-ray | Fractures, dislocations, bone alignment | 5-10 minutes | $100-$300 | First-line test for all knee trauma; rules out fractures before stress testing |
| MRI | Ligaments, menisci, cartilage, bone bruising, soft tissue | 30-60 minutes | $500-$3,000 | Gold standard for soft tissue injuries; required before most knee surgeries |
| CT Scan | Complex fracture patterns, bone fragments, surgical planning | 10-15 minutes | $300-$1,500 | Used when X-rays show fracture but more detail needed; better for bone than MRI |
| Ultrasound | Fluid collections, some ligament tears, real-time assessment | 15-30 minutes | $200-$500 | Limited use in acute trauma; helpful for detecting effusions and some tendon injuries |
X-rays are always ordered first. They're fast, inexpensive, and immediately rule out fractures and dislocations. However, X-rays don't show ligaments, menisci, or cartilage. A normal X-ray doesn't mean your knee is fine.
MRI provides the complete picture. It shows ligament tears, meniscus damage, cartilage injuries, and bone bruising (microfractures not visible on X-ray). Insurance often requires failed conservative treatment before approving MRI, but motorcycle accidents usually justify immediate imaging due to high injury severity.
CT scans excel at showing complex fractures. When surgeons need to reconstruct a shattered tibial plateau or plan hardware placement, CT provides the three-dimensional detail they need. Some trauma centers use CT as the primary imaging tool for motorcycle crash victims.
Arthroscopy—inserting a camera into the joint—serves as both diagnostic tool and treatment. Surgeons can visualize damage directly and repair it during the same procedure. However, arthroscopy is invasive and typically reserved for cases where imaging is inconclusive or surgery is already planned.
Surgical vs. Non-Surgical Treatment Options
When Surgery Is Necessary
Complete ACL tears in active individuals almost always require reconstruction. The ACL doesn't heal on its own because it's bathed in synovial fluid that prevents clot formation. Without reconstruction, the knee remains unstable, increasing risk of meniscus tears and arthritis.
However, older, sedentary individuals sometimes skip ACL reconstruction. If you don't plan to return to pivoting sports or riding, and you can modify activities to avoid instability, conservative treatment is viable. Success depends on honest assessment of your activity goals.
Displaced fractures need surgical fixation. When bone fragments separate, they won't heal properly without hardware holding them in place. Displaced patella fractures, tibial plateau fractures with depression, and femoral condyle fractures typically require plates, screws, or both.
Bucket-handle meniscus tears that lock the knee demand urgent surgery. The flipped fragment blocks motion and can damage cartilage if left untreated. Surgeons either repair the tear (if it's in the vascular zone) or remove the damaged portion.
Multi-ligament injuries—two or more ligaments torn—usually require surgery. A knee with both ACL and MCL tears might heal the MCL conservatively but still needs ACL reconstruction. Three or four ligament injuries (knee dislocation) require complex reconstruction, often staged over multiple surgeries.
Conservative Treatment Approaches
Isolated MCL tears (Grades I and II) heal without surgery. The MCL has good blood supply and responds well to bracing and physical therapy. Grade III MCL tears are controversial; some surgeons repair them, others brace for six weeks and accept slight residual laxity.
Non-displaced fractures can heal with immobilization. A stable patella fracture with minimal separation might heal in a brace or cast over six to eight weeks. However, the patella needs to glide smoothly for proper knee function, so even small displacements sometimes warrant surgery.
Meniscus tears in the vascular zone can heal with activity modification and physical therapy. Small peripheral tears sometimes scar down on their own. However, most meniscus tears in motorcycle accidents are complex and involve the avascular zone, requiring arthroscopic treatment.
Partial ligament tears (Grade II sprains) often respond to bracing and rehabilitation. You'll spend four to six weeks in a hinged brace that allows controlled motion while protecting healing tissue. Physical therapy focuses on regaining range of motion, then strengthening, then proprioception.
| Treatment Type | Injury Severity | Recovery Time | Success Rate | Pros & Cons |
| ACL Reconstruction | Complete ACL tear | 6-9 months to sports | 85-95% return to activity | Pros: Restores stability, prevents arthritis. Cons: Major surgery, long rehab, 5-10% graft failure rate |
| Meniscus Repair | Peripheral meniscus tear | 3-6 months | 70-90% healing | Pros: Preserves meniscus, protects cartilage. Cons: Slower recovery than removal, restrictions on weight-bearing |
| Meniscectomy (Removal) | Complex avascular tear | 6-12 weeks | 90% pain relief initially | Pros: Quick recovery, immediate weight-bearing. Cons: Increases arthritis risk long-term |
| ORIF (Fracture Fixation) | Displaced fractures | 3-6 months | 80-90% union rate | Pros: Restores anatomy, allows early motion. Cons: Hardware complications, infection risk, may need removal later |
| Conservative (Bracing/PT) | Isolated MCL, non-displaced fractures | 6-12 weeks | 85-95% for appropriate injuries | Pros: Avoids surgery, lower cost. Cons: Longer initial immobilization, potential for residual instability |
What to Expect During Knee Surgery After a Motorcycle Crash
Surgical timing depends on soft tissue condition. Surgeons prefer to wait until swelling decreases and skin heals. Operating through damaged, swollen tissue increases infection risk and compromises healing. Most ligament reconstructions are delayed two to three weeks post-crash unless there's a locked knee or vascular injury.
Fractures, however, often require urgent surgery. Displaced fractures need fixation within days to prevent further cartilage damage and allow early motion. Open fractures (bone exposed through skin) are surgical emergencies requiring irrigation and stabilization within hours.
Arthroscopic procedures involve two to four small incisions. The surgeon inserts a camera and instruments to repair menisci, reconstruct ligaments, or remove loose bodies. ACL reconstruction typically uses either your own hamstring tendon or patellar tendon (autograft) or cadaver tissue (allograft). Hamstring grafts cause less anterior knee pain but may be slightly weaker. Patellar tendon grafts are stronger but can cause kneeling discomfort.
The surgeon drills tunnels through your tibia and femur, threads the graft through, and secures it with screws or buttons. The graft initially has minimal strength; it takes months for your body to incorporate it and restore full strength.

Author: Hannah Pierce;
Source: spy-delhi.com
Open reduction internal fixation (ORIF) for fractures requires larger incisions to access bone. The surgeon realigns fragments, then secures them with plates and screws. Tibial plateau fractures sometimes need bone graft to fill voids where bone was compressed. Surgeons harvest this from your pelvis or use synthetic substitutes.
Post-operatively, you'll wake with drains (to remove blood), a bulky dressing, and possibly a CPM (continuous passive motion) machine that slowly bends your knee. Pain is significant for the first 48 hours. Nerve blocks placed during surgery help, but expect to need prescription pain medication initially.
You'll start physical therapy within days. Early motion prevents stiffness, but you'll have weight-bearing restrictions. ACL reconstructions typically allow immediate weight-bearing but restrict pivoting. Fracture repairs may require six weeks of non-weight-bearing or partial weight-bearing depending on stability.
Hospital stays range from outpatient (arthroscopy) to three to five days (complex fractures). You'll need someone to drive you home and help for at least the first week. Crutches or a walker are necessary for several weeks.
Recovery Timeline and Rehabilitation Milestones
Weeks 1-2: Acute Phase
Focus on controlling swelling, managing pain, and preventing complications. Ice, elevation, and compression help reduce swelling. You'll perform ankle pumps and quad sets (tightening thigh muscle without moving knee) to maintain circulation and prevent muscle atrophy.
Range of motion work begins immediately for most injuries. Stiffness develops quickly in injured knees; waiting too long makes regaining motion difficult. Your therapist will passively bend and straighten your knee, gradually increasing range.
Wound care is critical if you had surgery or road rash. Watch for infection signs: increasing redness, warmth, foul drainage, or fever. Infections can destroy surgical repairs and cause permanent damage.
Weeks 3-6: Early Recovery
Weight-bearing progresses according to your specific injury. Meniscus repairs require six weeks of restricted weight-bearing because the repair needs time to heal. Fractures follow similar timelines. ACL reconstructions usually allow full weight-bearing but with a brace.
Physical therapy intensifies. You'll work on achieving full extension (straightening) first—this is crucial and often difficult. Flexion (bending) progresses more slowly. By week six, you should reach 120-130 degrees of flexion for most injuries.
Strengthening begins with isometric exercises, then progresses to resistance bands and light weights. Quad strength is essential for knee stability and often lags significantly after injury.
Months 2-3: Intermediate Phase
Most patients discontinue crutches and braces during this phase (unless you had meniscus repair or complex ligament reconstruction). Walking normalizes, though you may still limp when fatigued.
Therapy focuses on progressive strengthening, balance training, and proprioception (joint position sense). Single-leg exercises, balance boards, and perturbation training retrain your nervous system to control the knee.
You can typically return to desk work during this phase. Physical jobs require longer time off.

Author: Hannah Pierce;
Source: spy-delhi.com
Months 4-6: Advanced Rehabilitation
Sport-specific or riding-specific training begins. For motorcyclists, this means practicing the movements required to mount/dismount, shift gears, and control the bike. You'll work on agility, quick direction changes, and higher-impact activities.
However, you're not ready to ride yet. Ligament grafts are still maturing, and your neuromuscular control hasn't fully returned. An unexpected pothole or emergency stop could re-injure your knee.
Months 6-12: Return to Full Activity
Return to motorcycle riding typically occurs between six and nine months post-surgery for ACL reconstructions, sooner for meniscus-only procedures or conservatively treated injuries. Your surgeon will require specific strength and functional tests before clearing you.
Expect some ongoing swelling and discomfort for up to a year. Weather changes, long rides, or increased activity may cause temporary flare-ups. This is normal and doesn't indicate failure.
Full recovery—meaning you don't think about your knee anymore—takes 12 to 18 months for major reconstructions. Some people experience permanent changes: slight stiffness, weather sensitivity, or altered sensation around scars.
Frequently Asked Questions About Motorcycle Knee Injuries
Moving Forward After Knee Trauma
Recovering from a motorcycle accident knee injury tests your patience and determination. Unlike a broken arm that heals in a cast, knee injuries require active participation in rehabilitation. Your outcome depends as much on your commitment to physical therapy as on surgical technique.
Set realistic expectations. You'll likely regain full function, but your knee may never feel exactly like it did before the crash. Weather sensitivity, occasional swelling after long rides, and awareness of the injury during certain movements are common. These don't prevent riding or living fully—they're simply reminders of what your body survived.
Document everything if you're pursuing a legal claim. Photograph injuries, save all medical records, track every therapy appointment, and note how the injury affects daily life. Insurance companies minimize payouts, so thorough documentation protects your interests.
Consider gear upgrades before returning to riding. Knee armor in pants or separate knee guards won't prevent all injuries, but they reduce severity. Some riders add frame sliders or crash bars to their bikes to create distance between the motorcycle and their legs during a fall.
Finally, recognize that recovery isn't linear. You'll have setbacks—days when your knee swells inexplicably or therapy exercises that seem impossible. These don't mean you're failing. Healing happens in cycles of progress, plateau, and occasional regression. Trust the process, communicate with your medical team, and give yourself grace during the difficult days.
Related Stories

Read more

Read more




The content on this website is provided for general informational and educational purposes only. It is intended to offer insights and guidance on motorcycle accident insurance claims, settlement processes, liability issues, coverage limits, medical compensation, and related insurance matters, and should not be considered legal or financial advice.
All information, articles, and materials presented on this website are for general informational purposes only. Insurance policies, liability standards, settlement practices, and state regulations may vary by jurisdiction and insurer. The outcome of a motorcycle accident claim depends on the specific facts of the accident, available evidence, policy language, and applicable law.
This website is not responsible for any errors or omissions in the content, or for actions taken based on the information provided. Users are strongly encouraged to consult with a qualified attorney or licensed insurance professional regarding their specific motorcycle accident claim before making decisions about settlements, negotiations, or coverage disputes.