

Crashed motorcycle lying on its side on urban road at dusk with cracked helmet nearby and tire skid marks on asphalt
Motorcycle Accident Head Injury – Symptoms, Treatment, and Recovery Guide

Each year, motorcyclists die at rates 37 times higher per mile than car drivers, and here's the sobering part—most of these deaths trace back to head trauma. Cars give you a steel cage. Motorcycles? You're the crumple zone. Your head takes forces that would normally get absorbed by a vehicle frame, and that physics problem explains why brain injuries dominate motorcycle fatality statistics.
What you learn about these injuries—how they develop, what warning signs matter, which treatments actually work—directly affects whether you or someone you care about walks away whole or faces years of rehabilitation.
Types of Head and Brain Injuries in Motorcycle Crashes
Crash dynamics tell the injury story. Hit something at 30 mph on a bike, and you're dealing with forces your skull wasn't designed to handle. Research shows bone can take roughly 520 pounds of force before it cracks, but the deceleration when you hit pavement or a car door regularly exceeds that—sometimes by multiples.
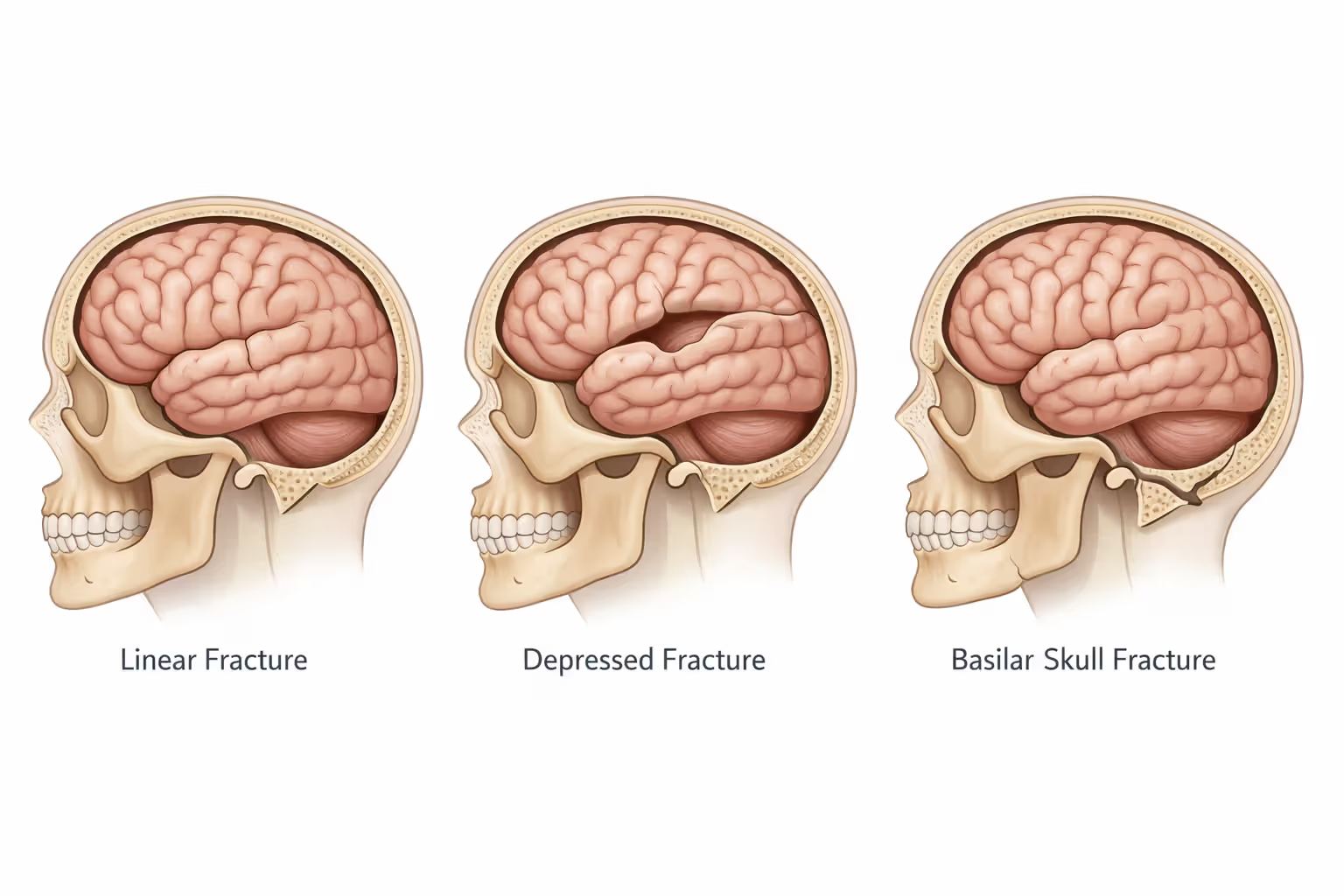
Skull Fractures and Surface Trauma
Linear fractures show up as clean breaks across the skull bone. Think of them as cracks without the pieces moving out of place. Doctors watch these for 4-6 weeks while the bone knits back together, though the real concern sits underneath—what happened to the brain during the impact that cracked the skull?
Depressed fractures drive bone pieces inward. That fragment now presses against your brain tissue, which doesn't tolerate pressure well. Surgeons often need to lift those pieces back into position, especially if they're pushing on critical areas.
Basilar fractures break the skull's foundation—the base where it connects to your spine. You'll see these when riders go face-first into something or catch their chin on an object during the crash. The telltale signs? Clear liquid (that's cerebrospinal fluid) leaking from your nose or ears, plus distinctive bruising that appears a day or two later: dark marks behind the ears or raccoon-eye bruising around both eyes without direct face impact.
Your scalp bleeds like crazy when cut because blood vessels pack the tissue densely. But here's the trap: people see all that blood, panic about the visible wound, and completely miss the fact that their brain just bounced around inside their skull.
Author: Olivia Bennett;
Source: spy-delhi.com
Traumatic Brain Injuries (TBI) – Mild to Severe
Medical teams use the Glasgow Coma Scale to grade brain injuries—it's a 3-to-15-point system testing whether you open your eyes, speak coherently, and move on command. Score 13-15? That's mild TBI, what most people call a concussion. Drop to 9-12, you're in moderate territory. Anything 8 or below means severe traumatic brain injury and usually an ICU bed.
Concussions happen because your brain floats in fluid inside your skull. When you're cruising at 35 mph and hit something solid, your skull stops instantly. Your brain keeps moving, slams into the skull's interior, then rebounds and hits the opposite side. That's equivalent force to falling off a three-story building and landing head-first. Neural connections shear and stretch during that violent motion.
Contusions are bruises on your actual brain tissue, with bleeding in the damaged area. The coup-contrecoup pattern is particularly nasty—say a car hits you from the left side. Your brain smashes against the left skull interior (coup injury), then whips back and crashes into the right side (contrecoup injury). You've now got damage in two separate brain regions from one impact.
Diffuse axonal injury represents the worst-case scenario in the brain injury motorcycle accident guide. Rotational forces—like when you're tumbling down the highway—tear nerve fibers throughout the brain. Half of severe DAI cases end in death. Survivors? They're typically looking at permanent disabilities because you've essentially shredded the wiring that lets different brain parts communicate.
Closed vs. Penetrating Head Injuries
Closed injuries leave your skull intact while your brain gets damaged internally. They're deceptive as hell. You stand up after the crash, shake it off, feel okay, and then six hours later you're unconscious on your bathroom floor because pressure's been building inside your skull this whole time.
Penetrating injuries mean something broke through—road debris, a piece of the bike, part of the car you hit. These bring obvious infection risks and almost always need emergency surgery, but there's a dark irony: the damage tends to follow a specific path rather than affecting the whole brain like closed injuries do.
Single-vehicle crashes (you versus the pavement) typically produce closed injuries. Multi-vehicle accidents increase your odds of penetrating trauma because there's more stuff flying around—metal, glass, cargo, plastic pieces—any of which can punch through your helmet and skull.
Warning Signs That Require Immediate Medical Attention
Brain injuries don't follow schedules. Some symptoms hit immediately. Others sneak up days later as bleeding accumulates or swelling squeezes your brain against the inside of your skull.
Call 911 right now if you see: any loss of consciousness (even seconds), seizures, clear fluid coming from nose or ears, pupils that aren't the same size, inability to recognize familiar people or places. Same urgency for severe headaches that worsen over time, vomiting repeatedly, slurred speech, or one side of the body going weak.
Doctors call it "talk and die" syndrome, and it's exactly what it sounds like. You're having normal conversations after the crash, maybe even joking with the paramedics. Then you collapse. What happened? Epidural hematoma—the artery running through your skull's middle (middle meningeal artery) tore during impact. Blood's been pooling between your skull and brain, and when pressure crosses a threshold, your brain function crashes fast. The classic pattern: brief unconsciousness right after the crash, then a "lucid interval" where you seem completely fine for anywhere from minutes to several hours, then rapid deterioration as the blood accumulation compresses brain tissue.
Watch for delayed symptoms in the 24-72 hour window: headaches that over-the-counter pills don't touch, confusion or gaps in memory, personality changes (suddenly irritable, depressed, or anxious when that's not your baseline), light and noise bothering you more than usual, sleeping way more or way less than normal, or trouble focusing on simple tasks.
Too many riders gamble on "wait and see"—especially if they're uninsured or facing a $5,000 deductible. That's Russian roulette with your brain. Swelling peaks 3-5 days after injury. Get ahead of it with medications, surgical decompression, or intracranial pressure monitoring, and you prevent secondary damage from oxygen deprivation. Wait too long, and damaged tissue becomes dead tissue.
Real case: 28-year-old rider in Oregon went down at 25 mph, slid across pavement, declined the ambulance because he "felt fine." Thirty-six hours later, his roommate found him unconscious in bed. CT scan showed subdural hematoma—bleeding between brain and skull. Emergency craniotomy saved his life but couldn't save his memory function. He'd been an electrician. Can't do that job anymore when you can't remember the code sequences or where you put your tools five minutes ago.

Author: Olivia Bennett;
Source: spy-delhi.com
How Helmets Reduce Head Injury Risk and Common Helmet Failures
According to the helmet injury motorcycle crash guide and NHTSA crash analysis covering more than 61,000 accidents, proper helmets cut death risk by 37% and prevent about 69% of head injuries. How? Three-part system: hard outer shell spreads impact force across a larger area, crushable foam liner absorbs energy (by destroying itself—that's why you replace helmets after crashes), and the retention system keeps everything positioned correctly when you're tumbling down the road.
Helmets reduce the risk of death by 37 percent and prove 67 percent effective at preventing brain injuries. Looking at 100 motorcycle rider deaths where no one wore helmets, 37 could have survived if they'd all been helmeted
— National Highway Traffic Safety Administration (NHTSA)
DOT certification requires helmets to handle impacts at speeds up to 13.4 mph without transmitting over 400 G-forces to the head inside. That protects you in many crashes, but not all. Speeds above 35 mph, multiple impacts (foam crushes once and stays crushed), or forces entering through gaps around the face shield or under the chin bar—these situations exceed what helmets can handle.
Half helmets and those "novelty" skull caps you see at rallies? Minimal protection. They're basically hard hats. Three-quarter helmets cover your skull crown and sides but leave your face and chin exposed—and research shows 19.4% of impacts hit the chin bar area on full-face helmets. Rear-end a car and you're going face-first into their bumper. That three-quarter helmet does nothing for you.
Helmets fail for predictable reasons. Wrong fit lets them rotate or fly off during impact. Proper fit: sits level on your head, covers your forehead to within an inch of eyebrows, doesn't move when you shake your head hard. Chin strap must stay fastened—26% of fatally injured riders who wore helmets had them separate during the crash because straps weren't secured.
Age matters too. Foam compresses over time, shells get brittle. Most manufacturers say replace every five years whether you've crashed or not. Buying used helmets? You're gambling that the previous owner didn't drop it (which compromises the foam internally without visible cracks) and is being honest about its history.
Even perfect helmets can't prevent every brain injury. Rotational forces causing diffuse axonal injury pass right through because the helmet moves with your head—it can't stop your brain from rotating inside your skull. Helmets excel at preventing skull fractures and reducing impact severity, but the motorcycle accident TBI guide makes this clear: you can't engineer away all TBI risk at high speeds.
Medical Treatment Timeline: From Emergency Room to Rehabilitation
Initial Assessment and Diagnostic Imaging
Emergency departments run standard protocols for motorcycle head trauma. First they handle ABCs—airway, breathing, circulation—while immobilizing your neck (30% of severe head injuries come packaged with neck injuries).
Glasgow Coma Scale happens within minutes of arrival. They test pupil light response, whether all four limbs move properly, and cognitive function by asking orientation questions (What's your name? Where are you? What day is it?).
CT scans happen fast—typically 15-30 minutes from door to images—for anyone scoring below 15 on the GCS, anyone who lost consciousness, anyone with amnesia about the crash, or anyone with "dangerous mechanism" written in their chart (high-speed crash, ejection from bike). CT shows skull fractures, bleeding, and swelling. What it misses: diffuse axonal injury and subtle contusions.
MRI gives superior brain tissue detail but requires 45-90 minutes and you lying still in a tube. Emergency departments reserve MRI for stable patients when CT findings don't match symptoms, or when surgeons need detailed maps for operation planning.
Blood work checks whether you have clotting problems (which make brain bleeds worse) and runs toxicology (alcohol and drugs affect treatment choices and become evidence in legal proceedings).
Surgical Interventions for Severe Cases
Neurosurgeons operate when imaging shows life-threatening bleeding or swelling. Craniotomy means cutting a skull section out to reach torn blood vessels or scoop out blood clots. Sometimes they leave that bone piece out (craniectomy) temporarily if your brain needs extra room to swell, then replace it weeks later once swelling resolves.
ICP monitoring involves drilling through your skull to place a pressure-measuring catheter. Normal intracranial pressure runs 7-15 mmHg. Above 20-25 mmHg, you need treatment: head elevation, controlled hyperventilation, osmotic diuretics like mannitol, or medically induced coma to reduce how much oxygen your brain demands.
External ventricular drains remove cerebrospinal fluid to relieve pressure when hydrocephalus (fluid backup) develops. The drain stays 5-14 days typically, with infection risk climbing the longer it remains.
Decompressive craniectomy—removing large skull sections—is the last resort when maximum medical management fails to control swelling. It saves lives at a cost: only 30-40% of patients achieve functional independence afterward. Survival doesn't equal the life you had before.
Long-Term Rehabilitation and Therapy Options
Acute rehab starts once you've stabilized medically, usually 1-3 weeks post-injury for severe cases. Inpatient rehabilitation facilities run intensive schedules—three-plus hours daily combining physical, occupational, and speech therapy.
Physical therapy rebuilds balance, coordination, and motor control. Many TBI survivors deal with hemiparesis (weakness on one side) or ataxia (movements that don't coordinate properly), which means relearning how to walk steadily and building strength back up.
Occupational therapy retrains daily activities: getting dressed, cooking meals, managing medication schedules. Cognitive rehab addresses memory, attention, and executive function deficits. When full recovery isn't realistic, therapists teach compensatory strategies—smartphone alarms, written schedules, environmental modifications like labeled drawers.
Speech-language pathology tackles communication disorders (aphasia where words won't come, dysarthria where words slur together) and swallowing dysfunction called dysphagia. About 25-30% of moderate-to-severe TBI patients can't swallow safely, requiring modified food textures or feeding tubes.
Neuropsychological testing at 3-6 months documents cognitive function objectively. These batteries measure processing speed, memory, attention span, and problem-solving ability, creating baselines for disability determinations and back-to-work decisions.

Author: Olivia Bennett;
Source: spy-delhi.com
Recovery varies wildly. Mild TBI symptoms usually resolve within three months, though 10-15% develop post-concussive syndrome with symptoms persisting beyond a year. Moderate TBI patients see the most improvement within 6-12 months but may continue gradual gains for 2-3 years. Severe TBI recovery stretches over years, with most gains concentrated in the first six months, then progress slows considerably.
Financial and Legal Considerations After a Motorcycle Head Injury
Author: Olivia Bennett;
Source: spy-delhi.com
Medical bills for motorcycle accident head injury cases start around $85,000 for mild TBI and climb past $3 million for severe injuries requiring lifetime care. Initial hospitalization alone averages $38,000-$150,000 depending on ICU days and whether you needed surgery. Inpatient rehab costs $1,500-$2,500 daily for stays lasting 2-6 weeks.
Long-term expenses pile up through outpatient therapy ($150-$300 per session, 2-3 times weekly for months), medications (anticonvulsants, antidepressants, pain management), assistive equipment (wheelchairs cost $2,000-$30,000 depending on type, hospital beds, lift systems), home modifications (ramps, wider doorways, accessible bathrooms), and lost income. Severe TBI survivors lose an average of $151,000 in lifetime earnings—many can't return to their previous jobs, period.
Insurance coverage gets complicated fast and rarely covers everything. Personal Injury Protection in no-fault states covers initial medical bills regardless of who caused the crash but caps at $10,000-$50,000—gone in days with serious injuries. Your health insurance might deny claims saying auto insurance should pay first, creating coverage gaps while insurers argue about whose responsibility it is.
Liability determination examines traffic violations, who had right-of-way, comparative negligence percentages, and sometimes just plain anti-motorcycle bias. Twelve states still use pure contributory negligence rules where if you're even 1% at fault, you recover nothing from other parties. Most states use comparative negligence, reducing your award by your fault percentage.
The at-fault driver's liability coverage should cover damages beyond what your insurance pays, but state minimums ($25,000-$50,000 in many states) barely scratch the surface of severe head injury costs. Underinsured motorist coverage on your own policy fills these gaps—if you bought adequate limits beforehand.
Statute of limitations gives you 2-3 years typically from the crash date to file suit, though some states extend deadlines when injuries weren't immediately apparent (discovery rules). Miss that deadline and your legal rights evaporate permanently.
Personal injury attorneys become essential when injuries involve hospital admission, permanent impairment, or fault disputes. Most work on contingency (33-40% of whatever you recover), so no upfront costs. Getting an attorney involved early preserves evidence—crash scene photos, witness contact information, helmet and vehicle inspections—that disappears quickly.
Settlement talks usually begin after you reach maximum medical improvement, when doctors determine your final prognosis. Accept early settlement offers before understanding your full injury picture, and you'll likely get inadequate compensation. Insurance adjusters push hard for quick settlements, before you lawyer up.
Third-party liability can extend beyond the driver to road maintenance agencies (crashes caused by potholes or poor road design), vehicle manufacturers (defective motorcycle or car parts), or even bars and restaurants (overserving alcohol to the driver who hit you). Finding every liable party with insurance or assets increases your potential recovery.
Factors That Influence Head Injury Severity in Motorcycle Crashes
Different crash variables combine to determine whether you walk away, spend weeks in rehab, or never wake up:
| Variable | Minor Outcome | Moderate Outcome | Severe Outcome | Critical/Fatal Outcome |
| Impact Speed | Below 20 mph | 20-35 mph range | 35-55 mph range | Exceeding 55 mph |
| Helmet Type | Full-face DOT/SNELL rated | Full-face DOT certified | Three-quarter or half-shell | No helmet or novelty cap |
| Impact Location | Glancing blow to side | Direct side or rear strike | Front or facial collision | Crown strike or multiple hits |
| Rider Position | Upright on motorcycle | Ejected and rolling | High-side ejection trajectory | Struck while on pavement |
| Object Struck | Flat pavement surface | Angled ground or curb | Vehicle body panels | Fixed objects (poles, trees) |
| Road Surface | Dry asphalt | Wet pavement | Gravel or dirt surface | Concrete barriers |
| Other Vehicle Type | None (solo crash) | Passenger car | SUV or pickup truck | Large commercial truck |
Individual factors matter less than how they combine. Crash into a car door at 30 mph wearing a full-face helmet? Probably mild concussion. Same speed into a telephone pole without a helmet? Fatal in most cases.
Speed drives severity because kinetic energy increases exponentially—double your speed and you quadruple the impact energy. The head trauma motorcycle accident guide emphasizes survival rates plummet above 45 mph regardless of helmet quality.
Impact angle determines force distribution. Glancing impacts let some energy dissipate as you slide, while perpendicular impacts deliver full force to a concentrated point. Riders who "lay the bike down" before hitting something often fare better than those who strike objects while still upright on the motorcycle.
Fixed object collisions—utility poles, trees, concrete barriers—transfer maximum energy directly to you. Crashing into vehicles allows some energy absorption through vehicle deformation, though SUV and truck height mismatches often put their bumpers at head level.
Frequently Asked Questions About Motorcycle Head Injuries
Protecting Your Rights and Your Recovery
Motorcycle accident head injuries create challenges that cascade through medical, financial, and legal domains far beyond the initial crash moment. Severity ranges from concussions resolving in weeks to catastrophic brain damage requiring lifetime care. Understanding injury types, recognizing warning signs, and seeking immediate medical attention form the foundation for optimal outcomes.
Helmet use remains your single most effective protective measure, though no helmet eliminates injury risk entirely at high speeds or during severe impacts. The gap between medical bills and available insurance coverage traps many injured riders financially, making early legal consultation valuable for preserving rights and maximizing recovery options.
Recovery timelines stretch longer than most riders anticipate. Mild injuries may resolve quickly, but moderate to severe TBI demands months to years of rehabilitation with uncertain final outcomes. Patience with recovery process, compliance with therapy recommendations, and realistic expectations about residual deficits help injured riders and families navigate the difficult path forward.
Document everything from day one—medical records, expenses, symptom diaries, crash evidence. These records support both treatment decisions and legal claims. Decisions made in the first days and weeks after a motorcycle head injury often determine recovery quality and financial stability for years ahead.
Related Stories

Read more

Read more




The content on this website is provided for general informational and educational purposes only. It is intended to offer insights and guidance on motorcycle accident insurance claims, settlement processes, liability issues, coverage limits, medical compensation, and related insurance matters, and should not be considered legal or financial advice.
All information, articles, and materials presented on this website are for general informational purposes only. Insurance policies, liability standards, settlement practices, and state regulations may vary by jurisdiction and insurer. The outcome of a motorcycle accident claim depends on the specific facts of the accident, available evidence, policy language, and applicable law.
This website is not responsible for any errors or omissions in the content, or for actions taken based on the information provided. Users are strongly encouraged to consult with a qualified attorney or licensed insurance professional regarding their specific motorcycle accident claim before making decisions about settlements, negotiations, or coverage disputes.